
Home / Ear Disease & Hearing Loss / Ear Pain
Ear Pain
Call +65 8125 3580
for 24 by 7 appointment
What are polyps in the ear due to?
Aural Polyps
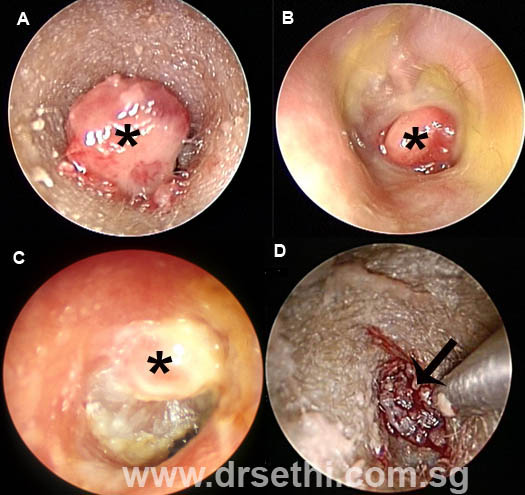
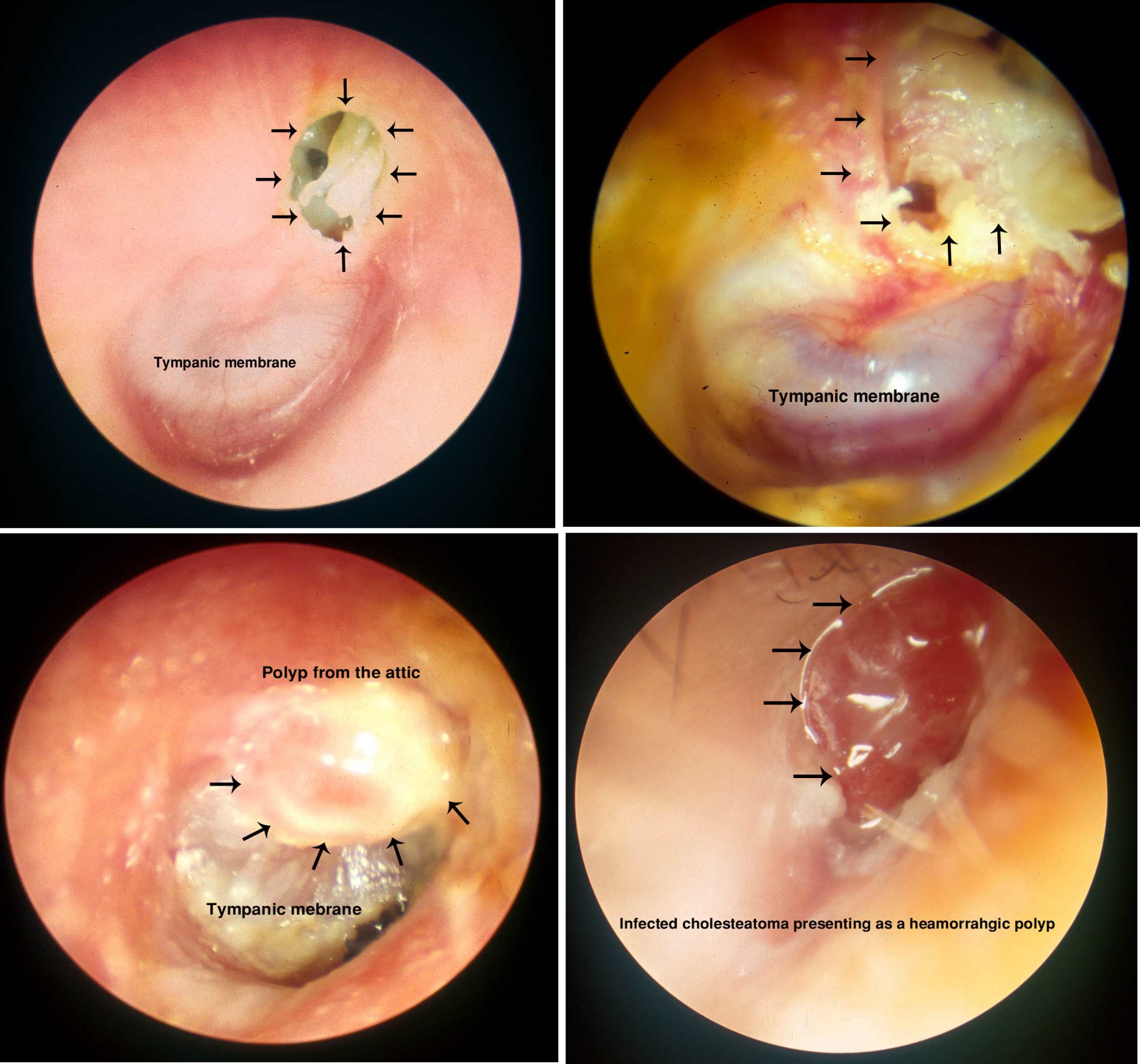
Aural polyps are benign, fleshy growths that arise from the skin or glands of the external ear canal or from the surface lining of the tympanic membrane. Aural polyps usually result from chronic irritation of the skin of the ear canal or eardrum. They can also arise from the middle ear and prolapse into the ear canal through a perforation in the tympanic membrane. Aural polyps can also be a manifestation of cholesteatoma. A polypoid (polyp looking) lesion, that bleeds easily may be a cancer arising from the skin of the ear canal. Very rarely, an aural polyp may be brain tissue prolapsing through the a defect on the roof on the mastoid cavity or the middle ear. The symptoms patients may present with include ear pain, discharge, bleeding, blocked ears or hearing loss.
A. Aural polyp causes by use of a sharp object to clean the ear canal. B. An aural polyps prolapsing through a perforation in the tympanic membrane. C. Infected cholesteatoma presenting with an aural polyp on oto-endoscopy. D: A vascular polypoid lesion suspected to be a malignancy. Biopsy confirmed a carcinoma arising from the skin of the ear canal.
Otoscopy or otoendoscopy examination will show the lesion. Further management will depend on what is suspected and may include a imaging studies such as CT scan of the temporal bone or a biopsy. If the polyp is caused by an infection and is arising from the ear canal it may be treated with topical and oral antibiotics. A biopsy or removal is indicated if it does not respond to medical treatment or malignancy is suspected When a cholesteatoma is suspected imaging studies like CT scan will help in determining the extent of the disease. Management of most cholesteaoma require surgical intervention. A biopsy is of the polyp is needed when a cancer is suspected.

A: arrow pointing to an aural polyp at the entrance of the left ear canal. B: MRI scan showed that the “aural polyp” was in fact brain tissue that was herniating into the ear canal and presenting as an aural polyp
Cholesteatoma
What is a cholesteatoma?
Fret not! A cholesteatoma has nothing to do with your cholesterol levels. It is a condition associated with the ear. As you may already know that the human ear is divided into three parts, 1. The outer ear, 2. The middle ear, 3. The inner ear. The outer ear is the pinna and the ear canal. Separating the ear canal from the middle ear is the tympanic membrane or the ear drum. The ear canal and the side of the ear drum facing the ear canal is lined by the skin. As anywhere else on our body, the ear canal skin also sheds squames. This shed skin is cleared out of the ear canal by a self-cleaning mechanism whereby the shed skin slowly migrates out of the ear canal and drops off outside. This mechanism also prevents excessive accumulation of wax with in the ear canal. The middle ear and the side of the ear drum facing the middle ear on the other hand is lined by mucus membrane similar to the back part of the nose. The middle ear connects to the back part of the nose also (nasopharynx) through a tube called the Eustachian tube. The main function of this tube is to keep the pressure of the middle ear the same as the external atmosphere. To be able to efficiently conduct sound from the ear canal to the inner ear it is required that these pressures be the same. The Eustachian tube also provides drainage to the middle ear. In patients with poor Eustachian tube function there is a persistent negative pressure in the middle ear causing the ear drum to gets sucked into the middle ear which now behaves like a vacum. This “sucking in” effect or retration is more likely to occur at a weak area of the ear drum. That weak area is called the “pars flaccida”. The pars flaccida is a very small area on the upper part of the ear drum. This retracted part of the ear drum form a small pouch. The shed skin within this pouch is not able to be cleared and keeps on collecting within forming a sac or a cyst which has now formed a “cholesteatoma”. Over time this cholesteatoma continues to grow. Initially it grows along the paths of least resistance invading the nicks and corners of the middle ear. The condition does not happen overnight. It may take years to develop. The patient initially has no or minimal symptoms. Attention is drawn to the ear, when the cholesteatoma gets infected and the the ear starts to hurt and discharge. Though not a tumour, the cholesteatoma behaves like one. It grows slowly destroying the structures around it.The cholesteatoma secretes several enzymes that destroy the bone around it. Destruction of the ossicles, the small bones in the middle ear results in hearing loss. It may erode into the inner ear destroying cochlea and the vestibular system and may extend as deep as the petrous apex. Destruction of the thin plate of bone that separates the middle ear from the brain predisposes the brain to serious complications such as meningitis and brain abscess. It may also break through the bone behind the ear and present as a skin abscess.Facial nerve, which supplies the muscles of the face may be destroyed resulting in paralysis of that side of the face.
What are the symptoms of a cholesteatoma?
In the early stages symptoms are minimal and often ignored. Patients usually present when the cholesteatoma gets infected. Typically the symptoms are, ear pain and ear discharge which is often scanty and foul smelling. The discharge may be blood stained. Patients may present with a complication such as mastoiditis, abscess, facial palsy and meningitis.
How is a cholesteatoma treated?
The treatment will depend on the presentation and the extent of the cholesteatoma. The ENT surgeon will take a detailed history and do a microscopic or endoscopic examination of the ear. Other investigations may include a hearing test and imaging studies such as CT scan of the temporal bone. Very small cholesteatomas that are still contained within a small sac which can easily be cleaned in the clinic may require nothing more than that. Larger cholesteatomas that have eroded the bone and the ossicles will need surgery to contain its spread. The objective is to remove all the cholesteatoma including the ossicles that have been involved and convert the ear into a wide cavity that can be cleaned in the clinic. Sometimes hearing may have to be sacrificed to achieve this goal. Though there are several modifications of the surgery, the common surgical procedures done for a cholesteatoma include atticomy, modified mastoidectomy, radical mastoidectomy and tympanomastoidectomy.
Why is my ear ringing?
“Doc, I have this ringing sensation in my ears…..” is a common ear related complaint that patients present with in my clinic. This ringing sensation is called “tinnitus”.
Tinnitus is defined as the “perception of sound that is not generated outside the body”. Some define it as a sensation of sound that does not exist. It may vary in its form and intensity. It is often described as ringing, humming buzzing or chirping. About 10-35% of the population may suffer from tinnitus at some point or the other. In fact it has been shown that if you place someone in a sound proof room for more than 20 minutes there is a 65% chance that person will experience tinnitus like sounds. Though its incidence may seem to be high but only about 10% of those having tinnitus are really troubled by it. That is still a significant number.
As there are several causes for tinnitus, the goals of the physician or the ENT doctor is to establish a diagnosis when possible and identify the treatable problems. Where the cause cannot be determined, it is important to assess the severity and determine if treatment is necessary.
A detailed history will include the duration, pattern, quality and severity of the tinnitus. Also included in the history is any significant medial history, associated symptoms related to the ears, and psychological issues and medication history. Aspirin is one medication that can cause tinnitus.
Examination will include an examination of the ears with the microscope and complete head and neck examination. A nasal endoscopy is done to rule out any pathology in the nose, sinuses and the nasopharynx. Tinnitus can be a presenting symptom of nasopharyngeal cancer.
An audiologic evaluation is essential to look for any associated hearing loss or middle ear pathology.
Imaging studies may include a computed tomography (CAT scan) of the temporal bone. CAT scan is excellent to study the bony anatomy of the ear. To look at the soft tissue anatomy a Magnetic Resonance is done. This is indicated particularly when the symptoms or the hearing loss are asymmetrical. If the patient has pulsatile tinnitus a Magnetic resonance angiogram or CT angiogram may be indicated. An arteriogram may be done when there is high index of suspicion of a vascular lesion.
Special Considerations:
- Clicking tinnitus may be due to Temporo-mandibular Joint dysfunction or stapedial myoclonus. Stapedial myoclonus is a condition that affects a small muscle in the middle ear.
- Pulsatile tinnitus: there are major vessels like the internal carotid artery, the internal jugular vein and the sigmoid sinus that come in close relationship with the ear. Increased vascular flow or lesions affecting these structures, such as glomus tumours, may cause pulsatile tinnitus. High intracranial pressure may also cause pulsatile tinnitus.
- Superior Canal Dehiscence: In this condition the bone overlying one of the semi-circular canals is weak or absent. It is usually associated with conductive hearing loss and vertigo
- Other conditions that can cause pulsatile tinnitus include dural AV fistulas and sigmoid sinus diverticulum.
- Acoustic Neuroma: this is a benign tumour arising from the 8th cranial nerve. Patients usually present with unilateral tinnitus, asymmetrical hearing loss, atypical vertigo and sudden hearing loss.
For cases where there is no obvious cause for the tinnitus and the patient is very troubled by the symptoms treatment for tinnitus include, hearing aids, tinnitus maskers, tinnitus habituation therapy and music based therapies. Medications may be helpful for some.
Not sure which form of ear pain you're experiencing? Speak to A/Prof Sethi to find out if the medical condition you have at +65 8125 3580. Or book an appointment with A/Prof Sethi for a consultation on your symptoms and treatment options.